
“We Will Be Giving…”
The subtle shift in language that changes everything about consent

I read a piece this week by Aaron Siri that, to a lot of people, felt shocking.
{kind=link}
To me?
It felt… familiar.
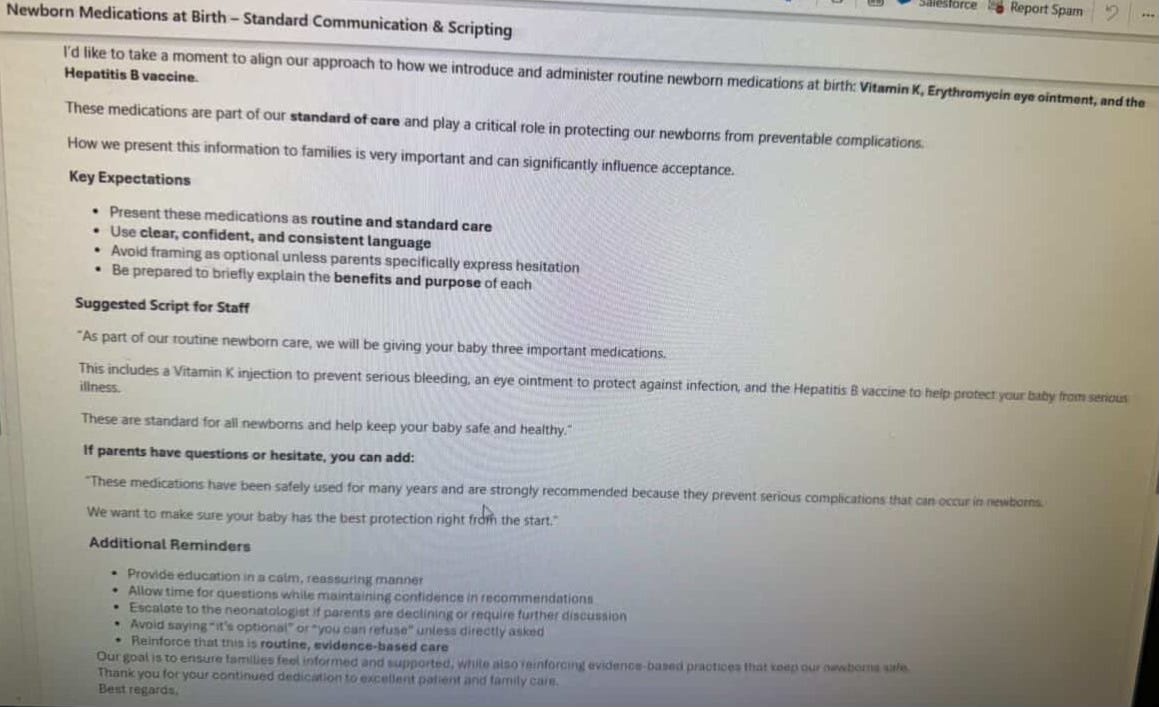
He shared internal guidance reportedly given to clinicians at Kaiser about newborn care—specifically around the Hep B vaccine.
The line that stood out:
“Avoid saying ‘it’s optional’ or ‘you can refuse’ unless directly asked”
and instead say
“we will be giving…”
He called it:
“the antithesis of informed consent.”
And he’s not wrong.
But here’s the part that may be harder to hear:
This didn’t surprise me at all.
Because this isn’t just one system.
This is how modern medicine has been trained to communicate—especially around vaccines.
From day one in training, we’re taught about something called “vaccine hesitancy.”
Not curiosity.
Not questions.
Not individualized decision-making.
Hesitancy.
It’s framed as one of the biggest threats to public health globally. According to the WHO and GAVI, vaccine hesitancy is one of the top 10 global health threats.

.And once you frame it that way…
Everything else follows.
The underlying assumption becomes:
👉 Everyone should get every recommended vaccine
👉 The default is yes
👉 The job is to increase uptake
So how do you do that?
You don’t ask.
You state.
“What would you like to do today?” or “Would you like to do any vaccines today?”
becomes
👉 “Today we’ll be doing…”
It sounds subtle.
It’s not.
Because language shapes perception.
And perception shapes decision-making.
The Kaiser document is the tip of the iceberg
The document Aaron Siri shared is far from earth-shattering and far from the only example of this. This is the default in medicine today. Let’s explore a few examples.
Center for Disease Control (CDC)
Let’s first explore how the CDC, the main body that creates the vaccine schedule for children tells practitioners to approach vaccine discussions.
Assume parents will vaccinate
Introduce the topic of vaccination with the assumption that most parents are planning to accept vaccines. State which vaccines the child needs to receive as though you presume that parents are ready to accept them during that visit. For example:
Instead of saying “What do you want to do about shots?,” say “Your child needs three shots today.”
Instead of saying “Have you thought about the shots your child needs today?,” say “Your child needs DTaP, Hib, and Hepatitis B shots today.”
A research study looking at health care professionals (HCPs) and parents’ interactions during vaccine visits showed that parents were more likely to express concerns when providers used language that asked parents about their vaccination plans. In this study, the presumptive approach resulted in significantly more parents accepting vaccines for their child, especially at first-time visits1.
Give your strong recommendation
If parents are not ready to vaccinate, then share your strong vaccine recommendation. Parents consistently rank their child’s doctor as their most trusted source for vaccine information. With this unique position, your strong recommendation is critical for vaccine acceptance. Clearly state your strong recommendation. If appropriate, you can add a brief supporting statement that uses a mix of science and anecdote, depending on what you think will be most effective with that parent. Share the importance of vaccines to protect children from potentially life-threatening diseases or talk about your personal experiences with vaccination.
For example:
“I strongly recommend your child get these vaccines today.“
“These shots are very important to protect him from serious diseases.”
“I believe in vaccines so strongly that I vaccinated my own children on schedule.“
“This office has given thousands of doses of vaccines, and we have never seen a serious reaction.”
Vaccine Saftey Institute
Next, let’s take a look at the Vaccine Saftey Institute by from Johns Hopkins
“The way providers introduce vaccination can be very influential on patients’ willingness to vaccinate. In particular, using a presumptive format when initiating vaccine conversations with patients has shown promise for increasing vaccine acceptance.1-9 The “presumptive approach” means expecting that your patients will vaccinate on time and should be the framework you use when you approach vaccination. Getting vaccines according to the recommended schedule should be the default choice for your patients. Instead of asking patients, “Would you like to get your influenza vaccine today?”, changing that simple question into the statement “It’s time to get your influenza vaccine today” can make a dramatic difference. The latter phrasing presumes that vaccination will occur, and therefore frames vaccination as the default.”
American Academy of Pediatrics
We can explore the American Academy of Pediatrics (AAP) website on this topic.
Same thing.
Presumptive Vs. Participatory Recommendations
Researchers found that pediatricians who provided a “presumptive recommendation” – informed parents that shots were due, rather than a “participatory recommendation” – asking what the parent thought about shots, were more likely to see parents accept vaccines.
Examples
Participatory:
“Do you want to vaccinate your child today?”
“What do you think about vaccines?”
“Would you like to hear about the vaccines we offer for today’s visit?”
Presumptive:
“Today your child is due for 2 vaccines. We will be giving MMR and Varicella.”
“It’s time for an annual influenza vaccine. Your child is old enough to receive either the inactivated shot or the live nasal spray.”
American Medical Association
How about this piece from the American Medical Association.

Tell patients they need to get the vaccine
Adult patients say the second biggest reason they don’t get an immunization is that a “doctor hasn’t told me I need it,” previously published research has shown.
Let’s do one more. How about this from NYS Dept of Health.

Optional Versus Announcement Recommendation
Optional: “Have you thought about what shots you’d like to get today?”
May unintentionally imply shot is not important or few people do it
20-30% vaccination rate in studies of both childhood and adolescent vaccine
High quality: “We have some shots to do today”
Implies shot is important and most people get it
70-90% vaccination rate in studies of both childhood and adolescent vaccines
Same thing over and over. This is just the default in modern medicine. So the Kaiser document is not “shock and awe” if you are paying attention.
I’ve seen this play out in real time.
A new parent, 24 hours into one of the most overwhelming experiences of their life, sitting in a hospital room running on no sleep, trying to process everything.
And someone walks in and says:
👉 “We’ll be giving this now.”
That’s not a conversation.
That’s a directive.
Now to be fair—this isn’t coming from a bad place.
Most doctors and nurses genuinely believe they’re doing the right thing.
They’ve been taught that these interventions are safe, effective, and important.
So in their mind, they’re helping.
But good intentions don’t replace informed consent.
Because real informed consent sounds like:
👉 “Here’s what this is”
👉 “Here’s why it’s recommended”
👉 “Here are the risks and benefits”
👉 “Here are your options”
👉 “What would you like to do?”
That last line matters.
A lot.
And here’s where things get uncomfortable.
When you remove that step—even subtly—you shift from:
👉 collaboration
to
👉 compliance
That’s a big deal.
I had a parent recently tell me:
“I didn’t even know I could say no. They just came in and did it.”
That’s not rare.
That’s happening more than people realize.
Again—this isn’t about being “for” or “against” vaccines.
It’s about something much more basic:
👉 The right to understand
👉 The right to ask
👉 The right to choose
Because if a medical decision is truly the right one… It should be able to withstand a conversation.
What concerns me most isn’t one guideline. It’s the mindset behind it.
When medicine becomes so focused on increasing compliance that it starts shaping language to avoid giving patients the full picture…
We have to pause. Because trust doesn’t come from scripting. It comes from honesty.
And here’s the irony.
The more we try to control the conversation…
The more trust we lose.
I see it every day. Parents aren’t asking fewer questions.
They’re asking more.
And when they feel like they’re not getting real answers…
They don’t lean in. They pull away.
So if the goal is better health outcomes…
This approach may actually be doing the opposite.
This is why I’ve changed how I practice.
Less:
👉 “This is what we’re doing.”
More:
👉 “Let’s talk about this.”
Because at the end of the day, my job isn’t to make the decision for you.
It’s to help YOU understand the decision.
That’s what informed consent is supposed to be.
Not a script.
A conversation.
The Real Question No One Is Asking
So here’s where I land on this.
While this may feel like a shocking revelation to many reading Aaron Siri’s piece (and I suspect he already knows this well and is highlighting it because the public doesn’t)… this isn’t shocking from inside medicine.
This is the system.
This is how clinicians are trained.
The default is to give.
The language is designed to move things along. And yes—it probably works in the short term. Some parents go along because they’re overwhelmed, or unsure, or don’t feel comfortable pushing back, or simply don’t realize they have a choice. And for a busy medical system, it’s certainly easier than sitting down for a 20+ minute conversation.
But I can’t help but wonder…Does it actually work long term?
Because I see the other side of this every day.
Parents who look back—especially on those first moments in the hospital—and feel like they didn’t fully understand what was happening. That they weren’t truly given a choice. And once that trust cracks… it doesn’t just affect that one decision.
It affects all of them.
And that’s the part I think mainstream medicine is missing. If anything, this approach may increase compliance in the moment… but decrease trust over time. And without trust, none of this works.
So I keep coming back to the same question:
If vaccines are as beneficial as we say they are… why do we need scripts on how to frame the conversation?
Why not teach doctors how to educate?
How to explain the benefits clearly, honestly, and respectfully?
How to actually practice informed consent?
Because in the end, that’s what this should be about.
Not convincing. Not scripting. Not managing hesitancy.
Just… giving people the information they need to make the best decision for their child.
The CDC and NIH spend a LOT of money every year studying how to coerce parents into vaccinating. They know that if they get them to accept everything at that first visit, they are less likely to balk down the road (unless the child has a bad reaction, which happens often).
Frankly, given the manipulation techniques used on parents, it's a wonder that any at all resist.